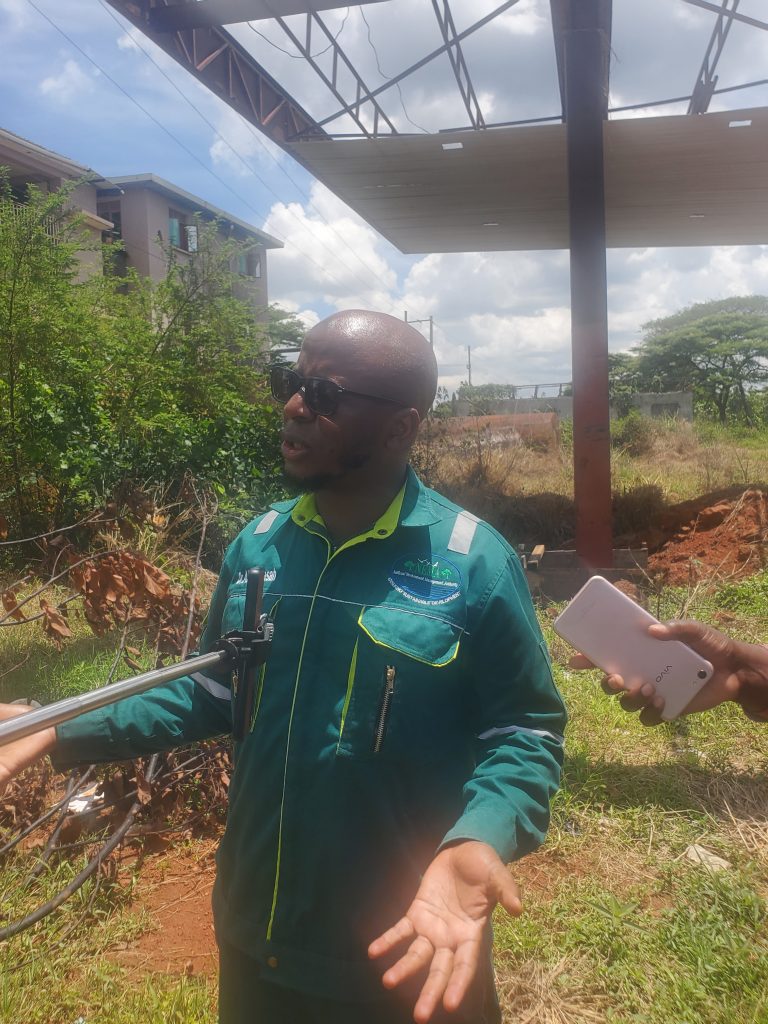
Midwife Apiyo Suzan is scanning a pregnant mother at Angaya HCIII using the POCUS (Mobile ultrasound machine)
POCUS is a portable ultrasound device used by healthcare providers to quickly assess and diagnose patients at the bedside.
By Chowoo Willy
Gulu District—At Angaya Health Centre III in Unyama Sub-County, 13 km away from Gulu city, the waiting area fills early. Pregnant women, some visibly weak, others quietly anxious, sit on wooden benches, awaiting their turn.
Inside a small examination room, midwife Apiyo Susan prepares a portable ultrasound machine. It is a recent addition but already indispensable. Gulu district previously had one ultrasound machine attached to Awach Health Centre IV.
Every day, she is scheduled to scan five to eight women. Some have come for routine antenatal checks. Others are not so fortunate.
“Sometimes they come when it is already too late,” Apiyo says. “You find infection has set in, there is bleeding, and the uterus is already affected.”

As she continues scanning patients throughout the day, the small device beside her represents more than just technology—it is a lifeline.
During a visit to the health unit on a Wednesday, she was found examining a woman from Ogul-Coope village who was five months pregnant.
“Your fetus is okay, but the baby is not lying in the correct position. This may change and become normal,” she said, reading the results from the portable scanner in front of her.
As of 2 July 2026, Apiyo had scanned 104 mothers. Those with mild complications are usually managed at the health unit, and referrals are always made for severe cases. In mid-May 2026, during her routine scanning, Apiyo diagnosed a woman with a molar pregnancy.
A molar pregnancy means a woman has all the signs of pregnancy, but there is no live fetus or live baby growing. The baby might have died in the early stage of pregnancy, but the placental tissues keep growing and become abnormally large in her uterus.
With it being beyond the capacity of the health unit to handle such an incident, the woman was referred to Gulu Regional Referral Hospital for further management.

“When we refer them, she benefits from evacuation.” She explains that. “So, when it is removed, she recovers and then has the opportunity to have another pregnancy later.”
The health expert attributes it to the practice of many women seeking care late from health facilities.
Gulu District Health Officer Dr. Canna Kenneth believes that “many women delay seeking care because services are far, expensive, or unavailable.
Dr. Canna stresses that by the time such women reach a facility, complications could have advanced.
For years, stories like these have defined maternal health and child healthcare in the Acholi sub-region. A subregion where hemorrhage contributed 48.5% to maternal deaths and postabortion complications contributed 9.4% in 2022, according to the MPDSR report.
Gulu District has Health Centre IV as the biggest health unit in the district, with 6 Health Centre IIIs and 12 Health Centre IIs serving the district. However, it is estimated that 33% of 100 pregnancies are always lost to abortion.
These lower-level health facilities, where most rural women first seek care, have lacked the tools to diagnose complications early. As a result, many women requiring post-abortion care (PAC) are referred to Gulu Regional Referral Hospital, often in critical condition.
Health workers estimate that at any given time, between five and ten women admitted to the gynaecological ward at the referral hospital are dealing with abortion-related complications—many of them preventable.
Dr. Pebalo Francis Pebolo, a gynaecologist at the hospital and a lecturer at Gulu University, attributes this to long distances to the health units in the rural setting for early diagnosis.
Dr. Pebalo says that most of them come having lost their pregnancies because they do not have money to transport them to health facilities, which has led many to bleed and develop complications.
“And if you don’t have the money, what will happen? You continue bleeding, you get an infection, and you get a blockage of the tube,” and he adds that, “at the end of the day, you are infertile because you stayed with a complication for long.”
For many women in Unyama and surrounding areas, the availability of free ultrasound services recently introduced has removed a major barrier to care. Previously, scans were only accessible in urban government health units and private clinics in town—often too expensive for rural families.
“People don’t have money,” Apiyo says. “Now they come here and get the service for free. The vulnerable are benefiting the most.”
Aol Monica, 40, is a resident of Agung Village, about 7 km from Angaya HCIII. She didn’t know that she was seven months and two weeks pregnant before the scan.

“I used to pay 22,000 Uganda shillings for a scan in private health facilities, but I was scanned here for free; the machine detected that I was seven months pregnant; I didn’t know this until I came here,” Aol adds.
Aol gave birth on the night of June 30, just as the scan had predicted.
“I was brought here in labour at midnight and gave birth exactly at 2 a.m.,” an excited Aol recounted.
The only ambulance given to the district recently to help in referral and transportation, most of the health workers struggle to fuel the vehicle. This further complicates responses.
Dr. Kenneth Canna, the district health officer, admits that the challenge always waters down their intervention to save lives.
Dr. Canna says it is very challenging to refer patients. “Sometimes you end up buying fuel from your pocket; sometimes you get tempted to ask patients to contribute a little to support their referrals.”
In a region where distance, poverty, and limited resources have long shaped maternal health outcomes, mobile ultrasound machines are quietly rewriting the story, one saved life at a time.
Technology revolutionising service delivery
In early 2026, Gulu District introduced five mobile Women’s Point-of-Care Ultrasound (POCUS) machines, the mobile ultrasound scan machines, across selected health centres. Ten midwives.
POCUS is a portable ultrasound device used by healthcare providers to quickly assess and diagnose patients at the bedside. The equipment was donated by Well on Their Way (WotU). A charity organisation in the USA.
The district has moved miles in piloting POCUS. This means a woman can receive an ultrasound examination at the same facility where she receives her routine care.
Dr. Canna says the introduction of mobile ultrasound technology is part of a broader effort to strengthen maternal health services.
“We are bringing services closer to the people,” he says. “This reduces delays in diagnosis and unnecessary referrals.”
The five machines have been distributed across the district and deployed at Angaya Health Centre III, Omel Health Centre III, Coope Health Centre II, Lugore Health Centre II, and Awach Health Centre IV.
From March to June 2026, the midwives carried out 306 obstetric point-of-care ultrasound examinations, with only 17% of those results being abnormal. These are 52 mothers.
That difference—between suspicion and certainty—is proving critical.
Dr. Canna says the mobile ultrasound machine is rapidly improving health coverage, as access to diagnostic services is a key indicator of a strong health system.
At Angaya HCIII, which serves the entire sub-county and sees up to 260 antenatal clients each month, the machine has become a frontline diagnostic tool. It is used not only to monitor pregnancies but also to detect complications that would otherwise go unnoticed until they become life-threatening.

“We use it for everything—normal pregnancies, but also when a mother comes with pain or bleeding,” Apiyo explains. “It helps us know exactly what is happening.”
In the neighbouring sub-county of Bungatira, the machine has supported medics in making two referrals out of the 52 scans conducted over the past three months at Coope Health Centre II.
Ayikoru Peace Maria, a midwife and the in-charge of the health unit, conducts a scan every Wednesday.
“We encourage them to undergo at least two scans to improve pregnancy outcomes.” She notes.
Dr. Pebalo describes ultrasound as a “game-changer” in this context because it strengthens the health system.
“It allows early detection of retained products, infections, and abnormal pregnancies like molar pregnancies. Without it, clinicians are working blindly.”
Medical experts say most women who experience spontaneous incomplete abortions are often unaware that they have lost their pregnancies.
Uganda continues to grapple with high rates of maternal deaths, many linked to preventable causes such as haemorrhage, infection, and unsafe abortion practices.
In rural districts like Gulu, the gaps in access and capacity are particularly pronounced. The district has a staff gap of 58%.
Mobile ultrasound machines alone will not solve these challenges. But they represent a critical step toward bridging the divide between rural health facilities and specialised care.
The hidden burden of unsafe abortions.
According to the World Health Organisation (WHO), unsafe abortions remain a major contributor to maternal deaths globally, accounting for about 8% of deaths worldwide, with 99.5% occurring in developing regions.
In Sub-Saharan Africa, unsafe abortions account for about 7% of maternal deaths, and the region has the highest maternal mortality ratio globally, about 542 deaths per 100,000 live births.
In Uganda, an estimated 300,000 abortions occur annually, with nearly 89% of healthcare facilities providing post-abortion care to treat complications from unsafe procedures.
One of the key challenges reported by health workers in Gulu District is that many women present late for antenatal services. Early antenatal attendance is critical in improving pregnancy outcomes.

Across the scanning points at the rural health units in Gulu district, among the most common findings are that they suffer from incomplete abortions—cases where a miscarriage or induced abortion leaves tissue inside the uterus.
“We scan and confirm if there are retained products,” Apiyo says. “If it is manageable, we treat here. preventing further complications.”
But not all cases are straightforward.
Two weeks earlier, Apiyo handled a patient who had attempted to terminate a pregnancy using suspected local herbs. By the time she arrived, her condition had deteriorated.
“She had fever, signs of infection, and the uterus was already in a bad state,” Apiyo recalls. “We could not handle it here. We referred immediately.”
Health workers say such cases are common in unsafe abortion attempts—and are exactly what early detection is helping to prevent.
Such cases—often classified as septic incomplete abortions—are among the leading causes of maternal deaths in low-resource settings, especially when care is delayed.
In 2025, a woman in Ogul-Coopil Village lost her life after suffering a ruptured uterus, unaware that she was pregnant until it was too late.
The LC III Chairperson of the sub-county, Justine Kidega, explained that the woman had been undergoing treatment for what she believed to be ulcers, not knowing that the pregnancy had developed in her fallopian tube.
“We are going to use this machine (scan) to sensitise the community on the importance of seeking ultrasound scans at health facilities so that we can prevent such tragedies,” he said.
The drivers of abortion-related complications in Gulu are complex. Health workers point to low uptake of family planning, incorrect use of contraceptives, and economic hardship.

“Some women conceive but are not ready to carry the pregnancy,” Apiyo says. “Others lose pregnancies due to malaria, which is very common here.”
At the community level, the reality is even starker.
“Post-abortion care is a big challenge in this area,” Kidega says. “Many women first try unsafe methods at home because they lack options.”
These methods—ranging from herbal concoctions to unregulated procedures—often lead to complications that could have been avoided with timely medical care.
Abortion in Uganda is largely illegal and heavily restricted, permitted only in circumstances where it is necessary to save the life of the pregnant woman.
A legal expert says restrictive abortion laws are pushing many women and young girls toward unsafe practices, often resulting in severe complications.
According to a human rights lawyer, Cinderella Alimuchan, fear of arrest drives women to seek local remedies instead of formal healthcare.
“As an individual, I may feel that since the law is against

abortion, I cannot go to Gulu Regional Referral Hospital,” she explains. “Instead, I turn to the grassroots, looking for herbs or other unsafe methods to terminate the pregnancy.”
She adds that fear is compounded by concerns that health workers may be legally compelled to report such cases to authorities.
“People fear going to the hospital because, in some circumstances, doctors are forced by law to report these cases,” she says.
Alimuchan notes that these restrictions have had far-reaching effects, not only on individuals but also on healthcare institutions.
A referral system under pressure.
According to the World Health Organisation (WHO), millions of unsafe abortions occur globally each year, with a significant proportion taking place in developing countries.
Research shows that approximately 8% of maternal deaths worldwide are linked to abortion, with 99.5% of these deaths occurring in developing regions.
In Sub-Saharan Africa, unsafe abortions accounted for about 7% of maternal deaths as of 2019. The region also bears the highest maternal mortality ratio globally, estimated at 542 deaths per 100,000 live births.
In Uganda, an estimated 300,000 abortions occur annually, representing about 14% of all pregnancies and a rate of 39 abortions per 1,000 women. Data further indicate that around 89% of healthcare facilities capable of providing post-abortion care treat complications arising from unsafe procedures (Guttmacher Institute, 2017).
Gulu Regional Referral Hospital is the main referral facility serving Acholi and neighbouring sub-regions. The hospital is overwhelmed by the growing number of women seeking post-abortion care.
Gulu Regional Referral Hospital receives between 5 and 6 women coming for post-abortion care daily. An average monthly estimate of 125 people.
Sr. Margaret Auma is the senior nurse in charge of the Gynaecology Department. Auma says the hospital continues to play a critical role in managing severe cases.
“We see septic abortions, heavy bleeding, and uterine injuries,” she says. “Many come very late.”
The hospital records cases of the recurrence of abortion as a result of some women getting pregnant before three months elapse to regain nutrients.
“We have seen some people who lose a pregnancy, and then after three months, they are pregnant, yet they need to replace this before they again get pregnant,” Dr. Pebalo notes.
Still, the referral system remains stretched, and delays persist. The medical expert says the hospital always goes beyond the ward to avoid the recurrence of abortion.
Sr. Margret reveals that they always advise women who come for post-abortion care to give time for the uterus to rest and recover before they can get another pregnancy.
“We educate them on hygiene, adherence to medication, and diet.” She says, “We give them the knowledge about family planning.”
Beyond the post-abortion care, these women are subjected to family planning methods, counselling, and adherence to medications.
Dr. Pebalo stresses that women who undergo abortion usually lose a lot of stored materials in terms of the nutrients they have stored in their bodies to build the fetus. When they conceive before they have fully recovered, they end up losing their pregnancies.
Despite the progress, the Manual Vacuum Aspirator (MVA) kits provided by the Ministry of Health are insufficient to meet the demand.
These kits are essential for emptying and cleaning the uterus during post-abortion care procedures. Usually, women had a septic abortion.
Gulu University’s Department of Obstetrics and Gynaecology has stepped in to support the hospital by supplying additional MVA kits.
According to Dr. Pebalo, the university has, over the years, supported the hospital in several ways, including generating locally relevant data, training medical personnel on harm reduction models, and providing critical supplies such as MVA kits.
Sr. Margaret commended the university for its timely support since 2020, emphasising the high demand for services.
Persistent challenges
The rollout of the ultrasound scan is not without challenges. Human resource shortages remain a critical bottleneck in the district.
At facilities like Angaya HCIII, a single midwife often handles multiple responsibilities—antenatal care, deliveries, family planning, immunisation, and now ultrasound scanning.
“I am the only midwife on duty most times,” Apiyo says. “I handle antenatal care, deliveries, family planning, immunisation—and now ultrasound scanning. It is overwhelming.”
She believes that with more staff, the full potential of the technology could improve service delivery in the district.
The district currently has 28 midwives deployed across different health units from 17 previously. But only 10 of them are trained in handling the ultrasound machine.
At Coope Health Centre II, Ayikoru is the midwife and the one in charge. She moves between the unit at Bungatira Subcounty and Pabwo HCIII in Owor Subcounty to scan women.
“Distance and transport cost are challenging; I only went there once,” Ayikoru explains.
The distance between the two health centres is about 5 kms. This reflects the typical 5km walking distance radius used to ensure women have access to an ultrasound scan.
Dr. Canna acknowledges the challenges but says efforts are underway to train more midwives in the use of Point-of-Care Ultrasound (POCUS).
He noted that the district is also seeking partners to support the expansion of the technology so it can reach more health facilities across the district.
A quiet shift in rural healthcare.
Despite these constraints, the impact of mobile ultrasound technology is already being felt.
For many women, cost has long been a barrier to accessing scans, which are typically available only in private clinics in urban areas.
“People cannot afford it,” Apiyo says. “Here, we provide it for free.”
This has not only improved access but also increased trust in the health system.
“We feel relieved; this machine is helping to save lives here,” Lalango Joyce, a resident of Loyo-boo, narrates.
Lalango, 67, a former traditional birth attendant in Layoboo village, has now become a community mobilizer for expectant mothers to go for antenatal services early.
Women who might otherwise delay or avoid care are now coming earlier—allowing complications to be detected and managed before they escalate.
In a region where maternal mortality remains a persistent challenge, such shifts matter.
Back in Angaya, Apiyo moves from one patient to the next, the soft hum of the ultrasound machine filling the room. Each scan tells a story—some reassuring, others urgent.
For the women who walk through her door, that small device can mean the difference between life and death.
And in a place where too many stories have ended in tragedy, that difference is everything.